Role of Inhibin B and Ratio of Luteinizing: Follicle-Stimulating Hormones in Phenotyping Polycystic Ovarian Syndrome
DOI:
https://doi.org/10.32007/jfacmedbaghdad.6642418Keywords:
Follicle stimulating hormone, luteinizing hormone ratio, Inhibin B, phenotypes, polycystic ovary syndromeAbstract
Background: Polycystic ovary syndrome is among the leading causes of fertility-related problems and menstrual irregularities in women of reproductive age. The granulosa cells of the developing pre-antral and antral follicles produce inhibin B, which triggers chemical responses in the ovaries. Inhibin B is most often observed in the follicular phase when levels peak early and then decline over time
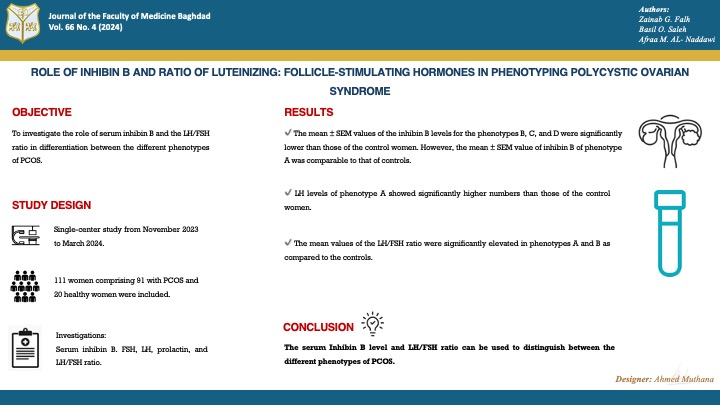
Objectives: This study was designed to investigate the role of serum inhibin B and the Luteinizing Hormone / Follicle Stimulating Hormone ratio in differentiation between the different phenotypes of polycystic ovary syndrome as well as to define the predominant PCOS phenotype.
Methods: This cross-sectional research was conducted in the Department of Biochemistry, College of Medicine, University of Baghdad from November 2023 to March 2024. The study included 111 women, ranging in age from 18-40 years. Among these, 91 women were diagnosed with polycystic ovary syndrome (PCOS) based on the 2003 Criteria for the Rotterdam Consensus, and the other 20 were healthy women. Investigations included serum levels of inhibin B using the Enzyme-Linked Immunosorbent Assay technique, follicle Stimulating Hormone, luteinizing Hormone and prolactin using Tosoh AIA-2000 Automated Immunoassay, to calculate the LH/FSH ratio.
Results: phenotype A was observed to be the predominant PCOS phenotype, while phenotype B was the rare form. The mean ±SEM values of the inhibin B levels for the phenotypes B (26.07±0.23 pg/ml, p=<0.001), C (25.96±1.68 pg/ml, p=<0.0001), and D (37.51±2.31 pg/ml, p=<0.0001), respectively, were significantly lower than those of the control women (57.68±2.07 pg/ml). However, the mean ±SEM value of inhibin B of phenotype A (50.46±7.12 pg/ml) was comparable to that of controls. The mean value of the LH levels of phenotype A (7.12±0.76 µIU/ml) showed significantly higher numbers than those of the control women (4.59±0.38 µIU/ml, p=0.03). Furthermore, the mean values of the LH/FSH ratio were significantly elevated in phenotypes A (p=0.001) and B (p=0.04) as compared to the controls.
Conclusion: Serum Inhibin B level and LH/FSH ratio can be used to distinguish between the different phenotypes of PCOS.
Received: July,2024
Revised: Aug.,2024
Accepted: Aug., 2024
Published: Dec.,2024
Downloads
References
1. Gupta M, Yadav R, Mahey R, Agrawal A, Upadhyay A, Malhotra N, et al. Correlation of body mass index (BMI), anti-mullerian hormone (AMH), and insulin resistance among different polycystic ovary syndrome (PCOS) phenotypes-a cross-sectional study. Gynecol Endocrinol. 2019;35(11):970-3. https://doi.org/10.1080/09513590.2019.1613640.
2. Shallal MM, Mahmood N, Hussein ZA. Total L-carnitine and insulin resistance in non-obese and obese Iraqi women with polycystic ovary syndrome. J Fac Med Baghdad. 2023;65(1):20-6. https://doi.org/10.32007/jfacmedbagdad.6512040.
3. Hatem A, O Saleh B, M Al-Naddawi A. Association between serum fructose level and insulin resistance in women with polycystic ovary syndrome: The effect of obesity. J Fac Med Baghdad. 2022;64(2):91-5. https://doi.org/10.32007/jfacmedbagdad.6421926.
4. M. Alawad Z. Level of follicular fluid vitamin D and embryo quality in a sample of Iraqi women undergoing IVF. J Fac Med. 2019;60(4):215-21. https://doi.org/10.32007/jfacmedbagdad.604758.
5. Mehra T, Sharma S, Zahra T, Jangir S, Gupta B. Correlation of Body Mass Index with Anthropometric and Biochemical Parameters Among Polycystic Ovary Syndrome Phenotypes. Indian J Clin Biochem. 2023;38(2):231-41. https://doi.org/10.1007/s12291-022-01042-y.
6. Group REPCW. Revised 2003 consensus on diagnostic criteria and long‐term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004;19(1):41-7. https://doi.org/10.1093/humrep/deh098.
7. Al-Naddawi AM, Rasheed MK, Ghalib MM. Association of Neuregulin-4 levels and body mass index with hyperandrogenism in Polycystic Ovary Syndrome patients. J Fac Med Baghdad. 2024;65(4). https://doi.org/10.32007/jfacmedbagdad.2140.
8. Gürsu T, Eraslan A, Angun B. Comparison of body mass index, anti-müllerian hormone and insulin resistance parameters among different phenotypes of polycystic ovary syndrome. Gynecol Obstet Clin Med. 2022;2(4):164-70.https://doi.org/10.1016/j.gocm.2022.10.002.
9. Ozay AC, Ozay OE, Gulekli B. Comparison of anti-müllerian hormone (aMh) and hormonal assays for Phenotypic Classification of Polycystic ovary Syndrome. Ginekol Pol. 2020;91(11):661-7. https://doi.org/10.5603/GP.a2020.0122.
10. Azziz R, Kintziger K, Li R, Laven J, Morin-Papunen L, Merkin SS, et al. Recommendations for epidemiologic and phenotypic research in polycystic ovary syndrome: an androgen excess and PCOS society resource. Hum Reprod. 2019;34(11):2254-65.https://doi.org/10.1093/humrep/dez185.
11. Hussein RA, Ali IN, Fahad NS. Estimation of Some Biochemical Parameters in Iraqi Infertile Women with Polycystic Ovarian Syndrome . Eur J Mod Med Pract. 2023;3(9):142-8. https://inovatus.es/index.php/ejmmp/article/view/1977.
12. Kalra B, Kumar A, Patel K, Patel A, Khosravi MJ. Development of a second-generation Inhibin B ELISA. J Immunol Methods. 2010;362(1-2):22-31.https://doi.org/10.1016/j.jim.2010.08.002.
13. Hassan HH, Ghazi SM, Nasif AS. Study of a Hormonal Assay in PCOS Patients with Type 2 DM and their Correlation with Inhibin B. Medico-Legal Updat. 2020;20(3). https://doi.org/10.37506/mlu.v20i3.1461.
14. Pratama G, Wiweko B, Asmarinah, Widyahening IS, Andraini T, Bayuaji H, et al. Mechanism of elevated LH/FSH ratio in lean PCOS revisited: a path analysis. Sci Rep. 2024;14(1):8229. https://doi.org/10.1038/s41598-024-58064-0.
15. Jozkowiak M, Piotrowska-Kempisty H, Kobylarek D, Gorska N, Mozdziak P, Kempisty B, et al. Endocrine disrupting chemicals in polycystic ovary syndrome: the relevant role of the theca and granulosa cells in the pathogenesis of the ovarian dysfunction. Cells. 2022;12(1):174. https://doi.org/10.3390/cells12010174.
16. Nisa KU, Tarfeen N, Mir SA, Waza AA, Ahmad MB GB. Molecular mechanisms in the etiology of polycystic ovary syndrome (PCOS): a multifaceted hypothesis towards the disease with potential therapeutics. Indian J Clin Biochem. 2024;39(1):18-36. https://doi.org/10.1007/s12291-023-01130-7.
17. Elsayed AM, Al-Kaabi LS, Al-Abdulla NM, Al-Kuwari MS, Al-Mulla AA, Al-Shamari RS, et al. Clinical phenotypes of PCOS: A cross-sectional study. Reprod Sci. 2023;30(11):3261-72.
https://doi.org/10.1007/s43032-023-01262-4.
18. Rabe-Hesketh S and Everitt BS. A handbook of statistical analyses using stata. Chapman & Hall/CRC, Taylor & Francis group. 2007 Fourth edition.
19. IBM SPSS Statistics 27 Core System User's Guide
20. Carmina E, Lobo RA. Comparing lean and obese PCOS in different PCOS phenotypes: Evidence that the body weight is more important than the Rotterdam phenotype in influencing the metabolic status. Diagnostics. 2022;12(10):2313.https://doi.org/10.3390/diagnostics12102313.
21. Malhotra N, Mahey R, Cheluvaraju R, Rajasekaran K, Patkar D, Prabhakar P, et al. Serum anti-mullerian hormone (AMH) levels among different PCOS phenotypes and its correlation with clinical, endocrine, and metabolic markers of PCOS. Reprod Sci. 2023;30(8):2554-62. https://doi.org/10.1007/s43032-023-01195-y.
22. Si M, Xu W, Qi X, Jiang H, Zhao Y, Li R, et al. Metabolic syndrome rather than other phenotypes in PCOS as a predictive indicator for clinical outcomes in IVF: comprehensive phenotypic assessment across all PCOS classifications. J Clin Med. 2023;12(15):5073. https://doi.org/10.3390/jcm12155073.
23. Obaid RM, Ali SH, Hameed HM. Correlation Between Serum Inhibin and FSH Levels in Women with Different Reproductive Disorders. Int J Res Appl Sci Biotechnol. 2022;9(3):256-61. https://www.ijrasb.com/index.php/ijrasb/article/view/414.
24. Fazil GJ, Sadig HA, Tofig MN, Ali IJ. The levels of inhibin A and inhibin B in PCOS patients. GSC Biol Pharm Sci. 2023;24(1):346-9. https://doi.org/10.30574/gscbps.2023.24.1.0302.
25. Farman MS, Akoul MA, Hamoode RH. Study of some hematological and hormonal changes in patients with (PCOS). Ann Rom Soc Cell Biol. 2021;2288-92. http://annalsofrscb.ro
26. Zhang F, Liu X ling, Rong N, Huang X wen. Clinical value of serum anti-mullerian hormone and inhibin B in prediction of ovarian response in patients with polycystic ovary syndrome. J Huazhong Univ Sci Technol [Medical Sci. 2017; 37:70-3.
https://doi.org/10.1007/s11596-017-1696-x.
27. Fawzy M, Lambert A, Harrison RF, Knight PG, Groome N, Hennelly B, et al. Day 5 inhibin B levels in a treatment cycle are predictive of IVF outcome. Hum Reprod. 2002;17(6):1535-43. https://doi.org/10.1093/humrep/17.6.1535.
28. Murat Ö, ÖZTÜRK HÇ. Anti-Mullerian hormone and HOMA-IR in different phenotypes of polycystic ovary syndrome on insulin resistance. Anatol Curr Med J. 2023;5(4):376-82. https://doi.org/10.38053/acmj.1323489.
29. Sharmin F, Mirza TT, Latif T, Islam FA, Shamsi S, Kabir MA, et al. Hormonal Parameters in Diverse Phenotypes of Polycystic Ovarian Syndrome. Mymensingh Med J MMJ. 2023;32(1):3-9. https://www.researchgate.net/publication/366837382.
30. Jamil AS, Alalaf SK, Al-Tawil NG, Al-Shawaf T. Comparison of clinical and hormonal characteristics among four phenotypes of polycystic ovary syndrome based on the Rotterdam criteria. Arch Gynecol Obstet. 2016; 293:447-56. https://doi.org/10.1007/s00404-015-3889-5.
31. Yilmaz M, Isaoglu U, Delibas IB, Kadanali S. Anthropometric, clinical and laboratory comparison of four phenotypes of polycystic ovary syndrome based on Rotterdam criteria. J Obstet Gynaecol Res. 2011;37(8):1020-6.https://doi.org/10.1111/j.1447-0756.2010.01478.x.
32. Arda Duz S, Tuncay G, Karaer A. Clinical and hormonal characteristics of women with various phenotypes of polycystic ovary syndrome. 2020; ;27(6):1626-30 https://doi.org/10.5455/annalsmedres.2020.02.125.
Downloads
Published
Issue
Section
License
Copyright (c) 2024 Zainab G. Falh, Basil O. Saleh, Afraa M. Al Naddawi, Ghada Mohammed

This work is licensed under a Creative Commons Attribution 4.0 International License.








 Creative Commons Attribution 4.0 International license..
Creative Commons Attribution 4.0 International license..